Can't be 9x. Some places are above 12%. That gives you a 108% infection rate.What variable are you currently using for asymptomatic or non-test confirmed COVID cases? At one point assumptions ranged up to 10x, but I’m not sure what the current assumption should be.
In September models were using 9x, but I wonder where it is at now?
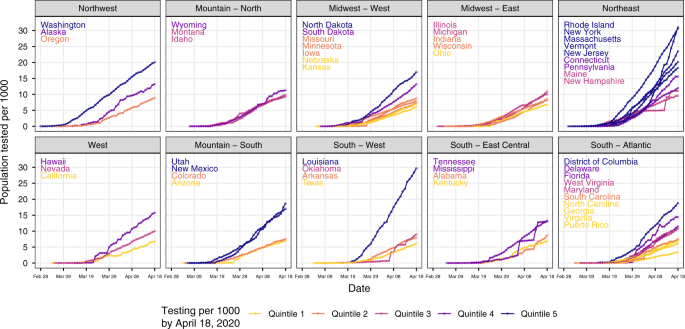
Substantial underestimation of SARS-CoV-2 infection in the United States - Nature Communications
Estimating the extent of SARS-CoV-2 infection in a population is challenging due to the limitations of testing. Here, the authors estimate that the true number of infections in the United States in mid-April was up to 20 times higher than the number of confirmed cases.www.nature.com
An OC study in the fall found 6x, for them..
Even 6x gives you above 100% infection rate for certain counties.
Going with 4 or 5x, depending on positivity rate. High positivity implies higher multiplier.





